Artificial intelligence (AI) has the potential to transform healthcare, and while there are several concerns about its safety and accuracy in clinical use, its presence is inevitable and improving patients’ outcomes.1
“It is not the strongest of the species that survives, nor the most intelligent. It is the one that is most adaptable to change.”
– Charles Darwin
At the annual SCCT meeting in Boston this past July, several companies presented their newest AI based technologies for evaluation of cardiac plaque, stenosis severity, flow limitation and inflammation.
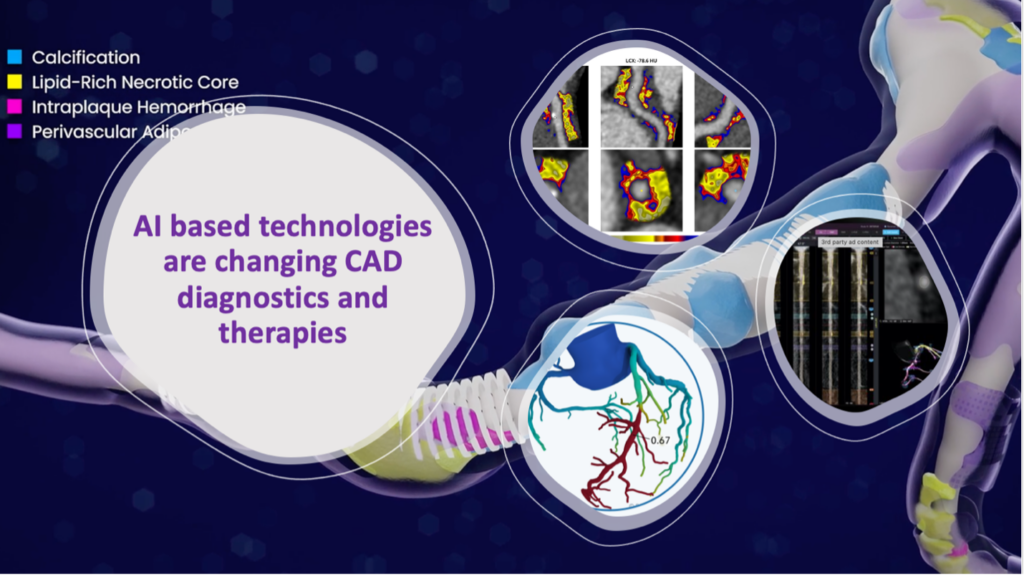
All these technologies are CT based, meaning they obtain information gathered by coronary CTA (CCTA). Some of them are in clinical use already, while others are emerging with novel imaging features that are changing the way we diagnose and treat coronary artery disease (CAD).
HeartFlow, was the first FDA approved company providing Fractional Flow Reserve derived from CCTA (FFRCT), a 3D functional analysis that supplements anatomical information from CCTA. This is equivalent to a stress test that can avoid layered testing, unnecessary radiation, and invasive procedures.2
For example, at a 1-year follow-up the PRECISE trial demonstrated that in comparison to a usual care pathway of stress testing or invasive angiography, a pathway centered on CCTA+FFRCT informed clinical decision-making such that clinical events were reduced by approximately 70%, non-invasive and invasive cardiac testing were reduced, preventive medication usage was increased, and the PCI:ICA ratio was improved.3
Multiple trials including the recent FISH&CHIPS found that adding FFRCT availability yielded clear improvement in endpoints within just 24 months. Among patients receiving a CCTA, those scanned during the period of FFRCT availability had 8% lower all-cause mortality, 14% lower cardiovascular mortality, 14% fewer additional non-invasive cardiac tests, 5% fewer additional invasive cardiac angiograms (ICA), Improved cath lab efficiency (higher ratio of PCI:ICA) and no increase in myocardial infarction rates.4
Results from RevealPlaque showed that HeartFlow’s Plaque Analysis demonstrated a 95% agreement compared to IVUS in quantification and characterization of total plaque volume.5
Cleerly provides qualitative and quantitative plaque analysis, including calcified, non-calcified and low attenuation plaque. Cleerly demonstrates high agreement with intravascular ultrasound (IVUS) for absolute measures of coronary lumen size to determine accurate stenoses measurements.6
Plaque stages can navigate physicians to initiate, intensify or de-intensify lifestyle interventions and medical management of patients with CAD.
Follow up scans demonstrate the effectiveness of statins for phenotypic plaque transformation through preferentially accelerating the calcification of plaque and reducing high-risk plaque development.7
Elucid Vivo offers the only AI based plaque analysis technology that was validated with histopathology. PlaqueIQ shows plaque characteristics and its vulnerability including lipid-rich necrotic core, calcifications, intraplaque hemorrhage and fibrous cap/perivascular adipose tissue. The company is also pursuing an indication for FFRCT derived from its PlaqueIQ technology to non-invasively measure extent of ischemia.8
Caristo diagnostics is an AI-enabled imaging solution that quantifies coronary inflammation and characterizes plaque, to help clinicians make more informed patient management decisions. Cari Analysis uses a novel imaging biomarker, the Fat Attenuation Index (FAI) to quantify coronary Inflammation. It provides an 8-year risk of a fatal cardiac event if left untreated, based on the FAI-Score values, the coronary atherosclerotic plaque burden, and the clinical risk factors.9
Other AI based algorithms (Bunkerhill) can obtain calcium score from lung cancer screening non-contrast chest CTs decreasing amount of radiation and cost for patients.
With the inevitable advancement of the AI technologies for diagnosis and treatment of heart disease, how adaptable is your cardiac program?
References
- http://doi.org/10.1056/NEJMoa1805971
- https://www.heartflow.com
- https://jamanetwork.com/journals/jamacardiology/fullarticle/2808765
- Fairbairn, et al. FFRCT In Stable Heart disease and CCTA Helps Improve Patient care and Societal costs. Presented at ESC 2023
- REVEALPLAQUE Study, presented at SCCT 2023
- Coronary CTA Plaque Volume Severity Stages According to Invasive Coronary Angiography and FFR. Journal of Cardiovascular Computed Tomography. Published March 2022.
- Progression of Atherosclerotic Plaque DetermIned by Computed TomoGraphic Angiography Imaging [PARADIGM]. Journal of the American College of Cardiovascular Imaging. Last Updated 2018.
- http://elucid.com
- https://caristo.com
- https://www.bunkerhillhealth.com